Trigeminal Neuralgia
Posted On April 6, 2020
- Unilateral electric shock like pain
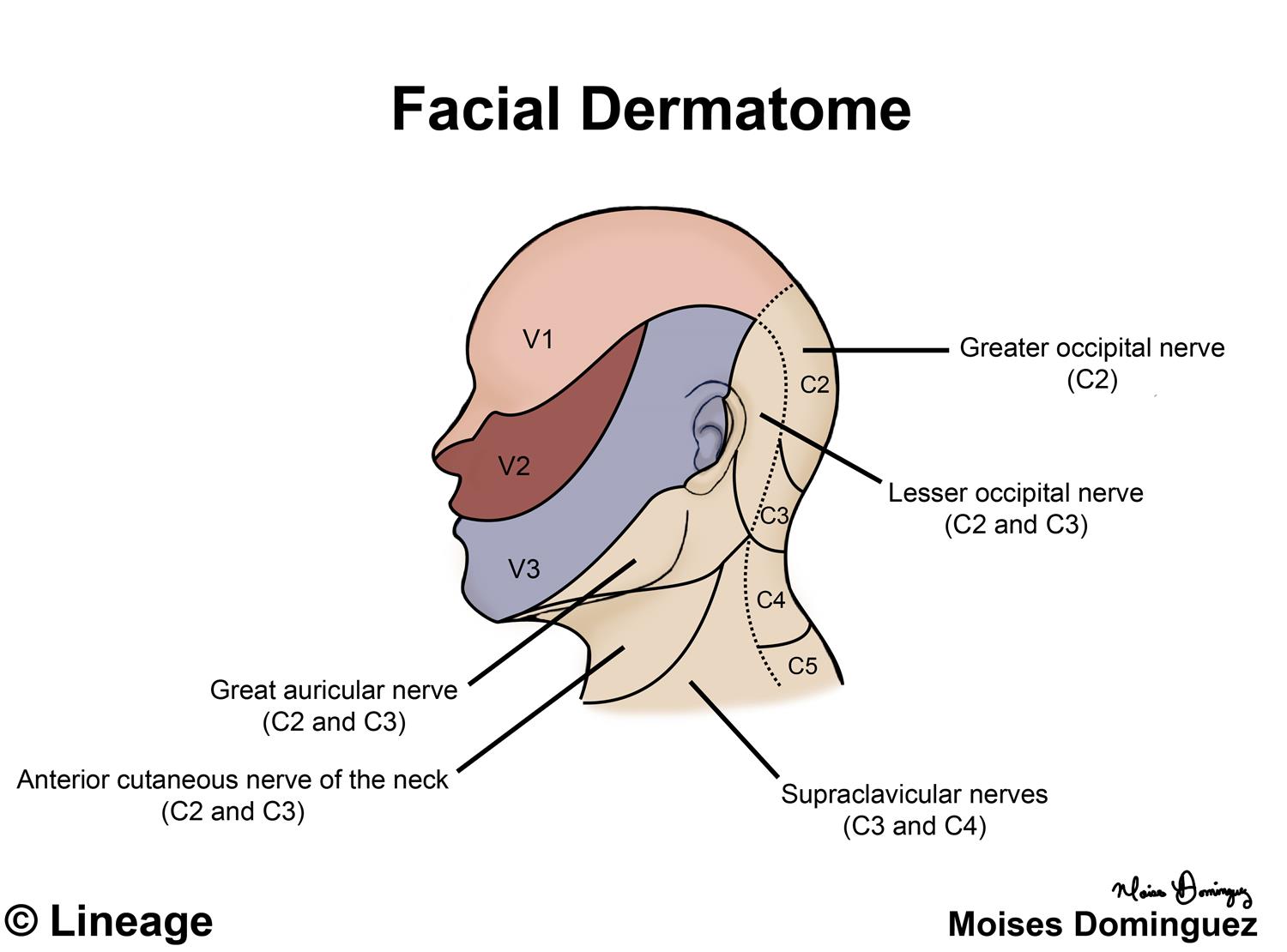
- involves one or more division of Trigeminal nerve
- over 80% caused by an aberrant loop of artery
- Less common: acoustic neuroma, meningioma, cyst, rarely an aneurysm or avm
- Treatment
- Carbamazepine, (Tegretol) most studied and effective. Start 100 to 200 mg bid, up to max of 1200 mg per day
- Oxycarbazepine (Trileptal), start 300 mg bid
- Possibly effective: baclofen, lamotrigine, pimozide
- baclofen 5 mg tid, upt to 60 mg per day
- lamotrigine 25 mg qd, increase by 25 mg daily every weekly, target dose 200 mg bid. Reduce dose if patient taking valproate.
- Pimozide, a dopamine agonist, seldom used due to potential side effects.
- Limited data: clonazepam, gabapentin, tizanidine, valproate
- Failed Carbamazepine: may try combination with gabapentin, lamotrigine, baclofen or tizanidine.
- Surgical treatment
- Microvascular decompression
- involves craniotomy
- initial pain relief 90%
- pain free rates decline to about 70% in 5 years
- Ablative procedures
- Microvascular decompression